Laminitis: Emergency care & management

Laminitis is a serious, painful, and sometimes life-threatening condition affecting the feet and hooves of horses and ponies. Effective emergency care and ongoing management are crucial for improving outcomes and minimising long-term damage. While there are many treatments and medicines recommended for laminitis, the most impactful interventions are often those (such as diet, farriery and ice therapy) that can be applied immediately at home, especially in the critical early stages. Here, we explore the stages of laminitis, the science and practice of early intervention (including ice-water therapy), and broader strategies for managing this challenging condition.
What is Laminitis?
Laminitis, sometimes called “founder”, is a severe, painful, and disabling condition that affects horses and ponies. It can be triggered by a range of factors, including nutritional imbalances, infections, hormonal disturbances, and mechanical stresses.
At its core, laminitis is an inflammation of the lamellae: these are delicate, leaf-like folds of tissue inside the hoof wall that anchor the inner hoof wall to the pedal bone (the lowest bone in the horse’s leg). When the lamellae become inflamed, they can weaken and tear apart, leading to partial or total breakdown of the strong bond that normally holds the pedal bone securely within the hoof capsule.
As the lamellae degrade, the pedal bone can become unstable and may rotate or sink within the hoof. This instability is extremely painful and often causes the horse to adopt a distinctive stance, stretching the forelegs out in front, tucking the hind legs underneath, and shifting weight onto the heels to relieve pressure on the damaged tissues.
Laminitis is a true emergency, and recognising the signs early is vital for giving your horse the best chance of recovery.
Understanding Laminitis: Stages and Progression
There are four stages in the onset and progression of laminitis:
Developmental: Damage is occurring deep inside the foot, but signs may not yet be visible.
Acute: Sudden onset of foot pain, heat, and a bounding digital pulse.
Subacute: Inflamed laminae but without total breakdown of the bond between the hoof wall and the pedal bone and collapse of the foot.
Chronic: Persistent lameness, further mechanical collapse of the foot, recurrent abscesses, and hoof wall deformation.
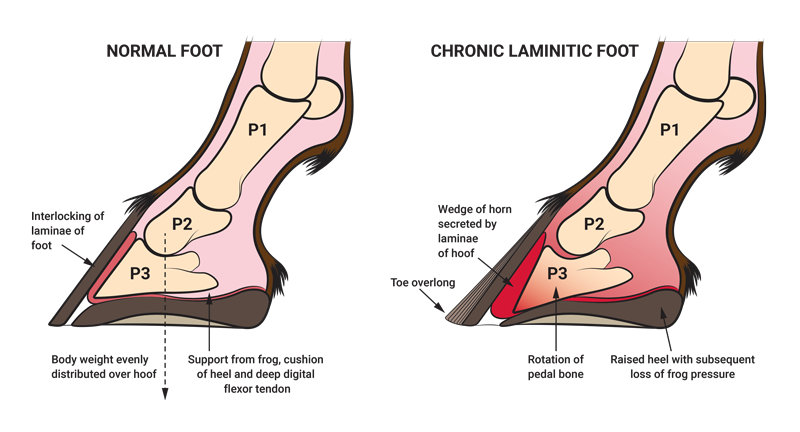
Diagram of Normal Foot vs Chronic Laminitic Foot. Courtesy of Southwest Equine Veterinary Group.
Most cases of laminitis occur due to disturbances in blood sugar and insulin secondary to high-carbohydrate feed, hay, or pasture. At-risk horses and ponies should be watched carefully every day, as laminitis is often difficult to detect, insidiously progressive and episodic, making identification of the developmental period difficult.
Developmental Stage
During the developmental stage of laminitis associated with high-carbohydrate feeds, blood glucose and insulin levels become dysregulated. Following a range of infections, including diarrhoea, foaling complications, metritis, pneumonia, colitis, or tying-up, it may be possible to anticipate the risk of laminitis, making prevention and early intervention more achievable.
The developmental stage of infection-associated (septic) laminitis overlaps with or follows the initial cause and lasts about 24 to 48 hours. Crucially, there may be no obvious signs of lameness or foot pain yet, but damage is already occurring within the hoof. This is the critical window when proactive measures, especially ice water therapy, can have the greatest impact and potentially prevent the disease from progressing. It is in this period that the greatest benefits of icing can be used.
If not halted, the developmental stage is followed by the acute phase, which usually lasts from one to seven days. If left unmanaged, laminitis can then progress to subacute or chronic forms. Subacute laminitis does not involve sudden collapse of the foot but progresses to persistent lameness, hoof wall deformation, and further mechanical breakdown.
Acute Stage
The acute stage is marked by the sudden appearance of clinical signs, most notably, foot pain, a bounding digital pulse, and heat in the hoof. Importantly, the stance of ‘front feet in front of the body’ taken to represent the classic ‘laminitis stance’ occurs in less than 50% of affected horses.
It is imperative to begin therapy as early as possible, ideally during the developmental stage, or at the very first sign of clinical foot pain. Early farrier and veterinary care make a significant difference to the outcome. If laminitis follows an infection, initiating ice-water therapy early is critical.
Subacute
The period of time beyond 72 hours after the onset of clinical signs during which the pedal (also called the coffin) bone remains undisplaced in relation to the hoof capsule.
Chronic
Recurrent episodes, complete failure of the union between the hoof wall and the pedal bone, detachment of the hoof wall, dislocation of the pedal bone, coronary band swelling and depression, divergent growth rings, change in hoof wall angle, flat/convex sole, widened white line and recurrent abscesses.
Digital Hypothermia: The Science and Practice of Ice Water Therapy
For inflammation‑associated laminitis, the single most effective treatment you can start at home is ice‑water therapy. It’s cheap, easy to apply, and the necessary equipment is probably already in your hands. The protective effects of ice water can prevent the development and progression of laminitis. Even after over 2000 years of study, the only proven therapy to prevent acute laminitis is the application of cold water from the knees and hocks down to the feet.
Digital hypothermia (immersing the legs in an ice slurry) during the developmental phase can help prevent the progression of laminitis and is increasingly recognised as protective for both prevention and treatment. The major results of ice therapy are:

Profound anti-inflammatory effects
Pain relief (analgesia)
Slowing of tissue metabolism, which reduces oxygen consumption by the damaged tissues and protects them from trauma and lack of oxygen
By reducing the requirement of cooled cells for oxygen, glucose, and other metabolites, inflammation is suppressed and cell survival is enhanced. Since laminitis changes are generally seen as irreversible, prevention in horses at risk and halting the progression of acute laminitis are key areas on which to focus.
How to Apply Ice Water Therapy
You don’t need fancy equipment; any method that keeps the lower limbs and hooves immersed in an ice-water slurry will work. For example, a 5-litre fluid bag secured with duct tape, or any sturdy bag that can hold an ice slurry around the legs, is effective. Refill the ice-water mixture every two hours to maintain a consistently cold temperature. Commercially available wader-style boots (modified to include the hoof) or rubber ice boots that reach just below the knee (carpus) and hock are also suitable options.
While cold gel wraps (at 4°C) can reduce surface temperature over the cannon bone for a few hours, they do not cool the deeper tissues as effectively as full ice-water immersion. Most commercial ice packs and cold-gel boots only lower hoof temperatures to around 20°C, but for laminitis, the goal is to reduce hoof wall temperatures to below 10°C. Achieving this requires cooling both the hoof and the limb, which also chills the blood entering the hoof and maximises the protective effect.
Although the exact “critical” temperature for laminitis prevention isn’t established, even a modest reduction in the temperature inside the hoof can be beneficial. Immersing the limb from just below the knees and hocks in ice and water is labour-intensive, but the benefits are significant. Continuous digital hypothermia, applied throughout the developmental period and for 24–48 hours after clinical signs resolve, can halt the progression of laminitis. In acute cases, cryotherapy may be continued for up to seven days after the first signs appear. When stopping, rewarm the limb gradually over 12–24 hours.

Concerns and Safety
A common concern is whether prolonged cooling could damage ligaments or tendons. However, studies show that even when tendon core temperatures are reduced to 10°C (22°C below normal), no harmful effects occur. Horses’ legs are remarkably resilient to continuous cold exposure, much like horses living in arctic conditions with legs immersed in snow. The cold-induced pain that humans feel at these temperatures does not appear to affect horses.
Important: If there is any suspicion of infection in the hoof (such as a subsolar abscess, septic arthritis, or seedy toe), avoid cryotherapy, as it may suppress the natural inflammatory response needed to fight infection.
Emergency Diet for all forms of laminitis
Diet plays a critical role in the early stages of laminitis, but feeding a horse with this condition can be challenging. Fortunately, there are excellent resources available, such as the Hoof Rehab Protocol and ECIR Group, that offer practical advice and evidence-based guidelines from leading veterinarians and farriers. Dr Kellon, a veterinarian specialising in equine nutrition, has developed an emergency diet specifically for horses affected by laminitis. This diet provides short-term guidance for owners managing a horse that has suddenly developed signs of the disease.
The emergency diet focuses on minimising sugars and starches while ensuring the horse receives essential nutrients. The recommended daily amounts are:

Grass hay at 1.5–2% of the horse’s current body weight, soaked to remove excess sugars.
Unmolassed beet pulp, rinsed, at 0.5–1 kg.
Iodised salt, 30–60 grams.
Magnesium oxide, 10–15 grams.
Vitamin E, 1000 mg (IU).
Linseed, 100 grams.
150 – 250g of a correctly-formulated vitamin and mineral balancer such as Jenquine all-4-feet®
It’s important to divide the total daily ration into at least three feeds per day to help stabilise blood sugar and insulin levels. This approach supports the horse’s recovery while reducing the risk of further metabolic disturbances.
For more detailed protocols and ongoing support, consult your veterinarian and refer to trusted resources such as the Hoof Rehabilitation Protocol or Equine Cushing’s and Insulin Resistance Group.
Additional Emergency Management Strategies
In the acute phase of laminitis (lasting up to 1 week), careful hoof care and support are essential to protect the damaged structures and promote recovery:
Hoof Trimming:
Ensure the foot is appropriately trimmed.
Avoid excessively long toes or low heels, as both can increase the risk of pedal bone rotation.
Bedding and Support:
Use deep sand bedding to provide uniform support to the foot.
Alternatively, pack the foot with a rubberised compound (such as plasticine) that moulds to the sole and frog, distributing pressure evenly.
Sole Cushioning:
Depending on the case, the shape of the sole (concave or flat), and the stage of laminitis, provide extra cushioning for the sensitive sole.
Options include a shoe, a glue-on pad, a pour-in support, or a hoof boot.
No boot fits every horse perfectly; daily monitoring for rubbing or pressure points is essential.
Movement and Rest:
Do not force the horse to move.
Encourage the horse to lie down as much as possible to reduce weight-bearing on the inflamed and fragile laminae, which connect the hoof to the pedal bone and support the horse’s weight.
Anti-inflammatory Medications:
Selection and use of anti-inflammatories should always be made in consultation with your veterinarian, as every case of laminitis is unique.
Nursing Care
Nursing care for horses with laminitis, especially those spending much of their time lying down, requires both attentive physical support and thoughtful attention to their mental well-being. It’s important to provide comfort and reassurance, ensuring the horse feels safe and cared for. Pain management is absolutely critical, and your veterinarian is the best resource for selecting and adjusting pain relief strategies tailored to your horse’s specific needs.
Because every case of laminitis is different, teamwork and clear communication between you, your vet, and your farrier are essential. Regularly assessing your horse’s condition and sharing your observations, such as changes in behaviour, demeanour, or comfort, will help guide ongoing treatment and allow your care team to make timely adjustments.
Exercise and Physical Therapy
Treatment for laminitis begins with eliminating or minimising any predisposing factors, using non-steroidal anti-inflammatory medications (NSAIDs) as advised by your veterinarian, providing strict stall confinement, and ensuring foot support that offers a biomechanical advantage.
Once the acute phase has passed, gentle movement becomes essential for both physical and psychological recovery. As soon as your horse can walk safely and comfortably without risking further damage to the foot, it’s important to introduce some form of exercise. For horses that remain sore or stiff, even a few minutes of slow walking on a soft, forgiving surface is a good starting point. The aim is to gradually increase the duration and intensity of exercise as your horse’s comfort and mobility improve.
Laminitis often causes tension in the shoulders, back, and flexor tendons, as the horse tries to keep weight off its painful feet. This can lead to soreness throughout the body, especially in the muscles and soft tissues of the shoulders, back, and hindquarters. In addition to gentle hand-walking, horses benefit from targeted exercises and physical therapy. For example, gently lifting the forelimb and slowly drawing it forward to extend all the joints in the limb can help relieve chronic tension from the hoof up to the back. This stretch should be performed slowly and fluidly, within the horse’s comfort limits, keeping the hoof close to the ground and in line with the shoulder. Avoid any forceful movements or pushing beyond the horse’s limits, as this can cause muscle tearing and further pain.
Other helpful exercises include gently leaning against the horse and shifting its weight from side to side or front to back without moving its feet. This slow, rhythmic rocking works with the natural elasticity of the tissues, providing a massaging effect that can reduce chronic tension and bring relief, even after a single session. Playful interactions, when safe, can also support both mental health and physical rehabilitation. If playing with other horses isn’t possible, you can bring a playful approach to daily exercises and interactions to keep your horse engaged and positive during recovery.
Concurrent Medical Issues
It’s essential to address any underlying medical conditions that may have contributed to the laminitis episode. The most common endocrine disorders linked to laminitis are Cushing’s disease (PPID) and Equine Metabolic Syndrome (EMS). Physical signs such as a cresty neck, enlarged fat pads along the crest, above the tail head, or in the sheath or mammary region, are often seen in “easy keepers” and are negatively correlated with insulin sensitivity. Obesity and regional adiposity not only increase the risk of laminitis but also place extra strain on the feet, further raising the likelihood of an episode.
Horses with cresty necks and laminitis may also have thyroid dysfunction, which can sometimes be secondary to a selenium deficiency. Selenium is vital for the liver to activate thyroid hormone, so your veterinarian may recommend testing for thyroid and selenium levels, as well as supplementing magnesium if needed. In cases where Cushing’s disease is suspected, your vet may also request blood tests for insulin, glucose, and cortisol.
Once the acute emergency has passed and the horse’s condition has stabilised, it’s important to transition to a correctly balanced diet, with weight loss as a goal if required. Many laminitic horses are especially sensitive to starch and sugars, so their diet should meet energy needs while keeping starch, sugars, and non-structural carbohydrates (NSC) low—ideally, NSC content should be 10% or less. For guidance on safe hay and pasture, resources such as Safergrass.org can be helpful.
Dietary management also includes deciding when, or if, affected horses can return to pasture. Obese or insulin-resistant animals should be kept off pasture for two to three months, allowing time for dietary restriction and increased physical activity to promote weight loss and improve insulin sensitivity. Feed hay with low NSC content (less than 10–12%) at 1.5% to 2% of body weight. Provide a suitable low-starch supplement (0.2–1.0 kg/day), fortified with biotin, antioxidants (vitamins C, E, and K), minerals (especially zinc, calcium, copper, iodine, and selenium), and amino acids to support healing. Flaxseed or canola oil (half to one cup per day, introduced gradually) can also be beneficial. If the supplement does not contain enough vitamin E, add 1–2 IU of vitamin E per 1 ml of oil.
Conclusion
Ultimately, successful management of laminitis relies on the dedication and teamwork of vets, farriers, and owners, supported by consistent, science-based care at home. While laminitis is a complex and often devastating disease, early intervention, especially with ice water therapy, can make a profound difference. Alongside vigilant management, attentive hoof care, and open communication with your veterinary team, you can give your horse the best chance of recovery and a return to comfort. Remember: prevention and swift action are key. If you suspect laminitis, act fast - start cooling, call your vet, and implement supportive management immediately.
References
Kullman et al (2013) Prophylactic digital cryotherapy is associated with decreased incidence of laminitis in horses diagnosed with colitis. Equine Veterinary Journal 46 (2014) 554–559 https://www.academia.edu/download/43246230/Prophylactic_digital_cryotherapy_is_asso20160301-8445-41eqek.pdf
Ryde L (2021) Cryotherapy of the distal limbs: an effective treatment for equine laminitis following onset of lameness? The Veterinary Evidence journal Vol 6, Issue 4 https://veterinaryevidence.org/index.php/ve/article/view/480
King C and Mansmann R (2004) Preventing laminitis in horses: dietary strategies for horse owners. Clinical Techniques in Equine Practice, 2004https://www.researchgate.net/profile/Christine-King/publication/244871277_Preventing_laminitis_in_horses_Dietary_strategies_for_horse_owners/links/63cee8f5d9fb5967c2fd6a88/Preventing-laminitis-in-horses-Dietary-strategies-for-horse-owners.pdf
Corder, M (2015) The Relationship Between Equine Diet and Presentation of Laminitis https://etd.ohiolink.edu/acprod/odb_etd/ws/send_file/send?accession=ksuhonors1431787834&disposition=inline
Dr Jennifer Stewart
BVSc BSc PhD Equine Veterinarian and Consultant Nutritionist
